Roy Wayne Chambliss, age 74, passed away on Tuesday, February 25, 2025, peacefully in his home. He will always be remembered as a loving husband, father, grandfather, great-grandfather, and friend to all who knew him. Wayne lived a life marked by kindness, dedication, and love for his family and the outdoors. His sense of humor and unwavering spirit left a lasting impression on all who knew him.
Wayne was born on May 16, 1950, in Gilmer, Texas, to Leonard Arthur and Josephine Crain Chambliss. He retired from Alcoa after many years of dedicated service and was a longtime resident of Daingerfield, Texas.
Wayne married the love of his life, Sherry Yvonne Edwards, in Texarkana, Texas, on June 12, 1992, and was a devoted husband. He was the co-owner of Kids First Co-Parenting Program. After retiring in Cuero, Texas, Wayne was a good neighbor who believed in lending a helping hand. He had a strong sense of right and wrong, always standing by his principles and guiding others with wisdom and integrity. Wayne lived life in the present, appreciating each moment as it came. He had a passion for gardening, woodworking, hunting, fishing, and playing card games.
Wayne is survived by his devoted wife, Sherry Chambliss; daughter, Ginger Caskey, and husband, Tommy; Robby Chambliss and wife, Ashley; Kyle Chambliss and wife, Jeannette; Mark SoRelle and wife, Pacifica; Craig Jones and wife, Geri; and Allison Jones and husband, Pete; and sister-in-law, Sharon Chambliss. His grandchildren include Kaen, Victoria, Carley, William, Brady, Riley, Gage, Blake, Ember, Joseph, Kelsey, and Willard. Great-grandchildren include Rosalie, Samuel, Bentley, Austin, and Janet.
He was preceded in his death by his parents, brothers Kenneth Chambliss and wife, Betty; Jerry Chambliss and wife, Pat; and Bill Chambliss.
A remembrance of his life will be held at Freund Funeral Home in Cuero, Texas, on Saturday, March 1, 2025. Visitation will be at 9 am, followed by a memorial service at 10 am with Dr. Glenn Robertson officiating. Wayne will be deeply missed but never forgotten. His legacy of love, laughter, and kindness will live on in the hearts of all who were blessed to know him.
Memorial contributions may be made to Tunnels to Towers Foundation, 2361 Hylan Boulevard, Staten Island, NY 10306.
You may sign the guestbook or send condolences at www.freundfuneralhome.com.
To plant Memorial Trees in memory of Roy Wayne Chambliss, please click here to visit our Sympathy Store






")

")
")

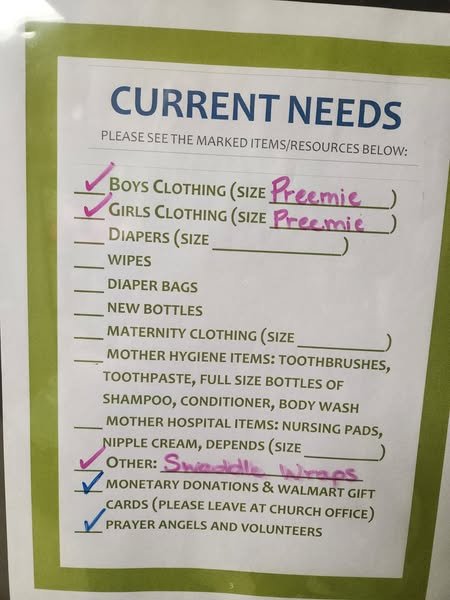 For more information, please contact Holy Cross Catholic Church in Yorktown.
For more information, please contact Holy Cross Catholic Church in Yorktown.